Peptide Protocols for Recovery & Performance
On a category that has more conversation than precision, and the questions we ask before we prescribe.
— Matthew Koucky · Hew Health · Vol I, Issue 04
A patient sat down last week and put his phone face-up on the desk. On it was a three-paragraph forum post about a peptide he had seen mentioned on a podcast. He wanted to know if it was something we could prescribe — and, more importantly, whether he should want it. That second question, increasingly, is the one we end up answering.
Peptide therapy has moved from a niche interest in sports medicine clinics into a category that patients now bring to us by name. Some of the names are reasonable. A few are oversold. A handful are entirely unsupported. The job, on our side of the desk, is to make those distinctions in plain English and without theater.
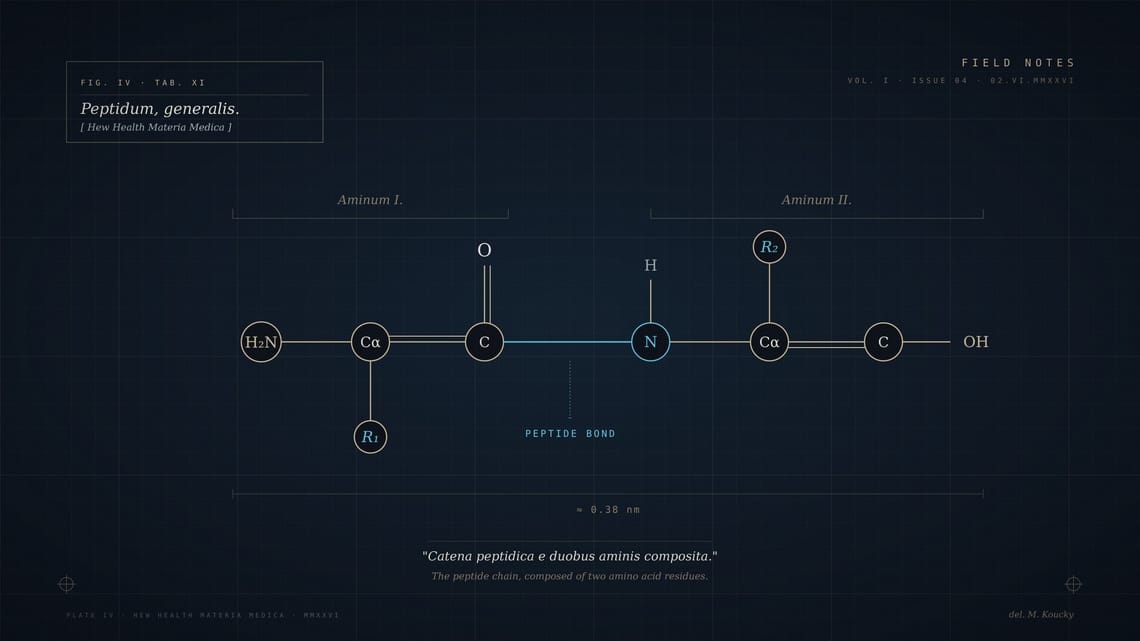
What we mean when we say peptide
A peptide is a short chain of amino acids — long enough to have a specific shape and signaling function, short enough to be synthesized cleanly and delivered precisely. The body uses peptides for nearly everything: appetite, sleep, immune response, wound healing, the way your heart adjusts during a long run. Synthetic peptides allow us to reintroduce or amplify specific signals that the body's own production may have dampened with age, stress, or illness.
The category is real medicine. It is also subject to the same hype cycle as any new tool — early enthusiasm, oversold claims, eventual settling into the place it actually deserves. We are somewhere in the middle of that cycle now.
The clinical questions, in order
Before any peptide is prescribed in our practice, the conversation runs through a short, deliberate sequence.
What problem are we solving? Recovery from a specific injury, sleep architecture, immune resilience, body composition, cognitive function? The answer to that question dictates everything downstream. The wrong peptide for the right problem is still the wrong intervention. We have learned to say this out loud, often, and early in the visit.
Is the symptom actually addressable here? Some recovery complaints are better answered by sleep work, training load reduction, or nutritional changes that take weeks rather than peptides that take months. Some are downstream of hormonal patterns that we would want to optimize first. A peptide protocol layered on top of a real endocrine deficit is a small lever pulled against a large door.
What is the realistic timeline? Recovery protocols often show something at four to six weeks. Body composition protocols are slower; expect eight to twelve. Sleep peptides are sometimes immediate, sometimes not at all. A patient who expects a peptide to work like an antibiotic — fast, on, off — is set up for a frustrating couple of months.
What does failure look like? We talk about what would convince us that the protocol is not working, and what we would do instead. This is a conversation a lot of practices skip. It is one of the most important ones we have.
What we actually prescribe
Our practice uses a narrow set of well-characterized peptides — the ones with the longest clinical history and the clearest mechanism. We do not chase novelty. We do not stack four peptides because the patient read a forum post that said stacking works. We use single agents at established dosing, observe for eight to twelve weeks, and reassess against the actual goal the patient came in with.
The categories that get prescribed most often in our practice are recovery and tissue repair, sleep architecture, body composition support adjacent to a broader weight management program, and, in some cases, immune resilience. Each category has one or two agents we trust enough to put a patient on. The list of agents we will not prescribe is longer than the list of agents we will.
A note on availability
Several peptides that were broadly available a year ago are now restricted or compounded-pharmacy only. This is not an emergency, but it is a logistical reality our patients should know about. We will tell you upfront what we can and cannot reliably source for the next six months, and we will not start a patient on something we cannot continue to supply.
The regulatory landscape on peptides is moving. We track it. When something changes that affects a patient's protocol, we let them know directly, not through a generic email blast.
Questions we keep getting
Is this performance-enhancing? If you compete in tested sport, the answer to that question matters more than the answer to any clinical question. Several peptides we use are on banned substance lists. We will tell you which and route the conversation accordingly. Cash-pay patients who are not in tested competition still get the same disclosure — it is the right framing either way.
Can I take this and stop my other medications? Almost never. Peptides interact with the broader medication picture, and a protocol that requires the patient to stop something else is a protocol with much higher coordination cost than we usually want to take on without a long discussion.
Will it show up on labs? Some peptides produce measurable shifts in standard labs; some do not. We tell the patient what to expect, and we time the labs to actually see what we want to see.
How long do I stay on? The answer is almost never indefinitely. Most of our peptide protocols are designed in cycles — on for a defined window, off for a defined window, reassess. The patients who do best are the patients who treat peptides as periodic interventions, not as maintenance medications.
What we don't prescribe, and why
There are peptides we have stopped prescribing — not because they were unsafe, but because the evidence base never caught up to the marketing. There are others we have never started prescribing for the same reason. The list shifts slightly each year.
The short version: if a peptide's strongest evidence is a podcast and a few anecdotes, we are not the practice that will write it. We are also not the practice that will dismiss it out of hand. The honest middle ground — we will watch the literature, we will tell you when we have changed our minds — is the only one that holds up over years.
The patient with the phone on the desk asked, finally, whether the specific peptide in the forum post was something we used. The answer was: not currently, for reasons we explained, and here is what we would offer in its place if his goal is what he described. He took the recommendation. The protocol is six weeks in. The labs at week eight will tell us whether we made the right call.
That is the honest version of how peptide medicine works in our practice. It is slower than the internet promises and steadier than the headlines suggest. Most things in optimization are.
⁂
Tags: Peptide Therapy · Recovery · Performance · Optimization
Author: Matthew Koucky
Category: Concierge Medicine
Read time: ~8 min
Field Notes is the editorial blog of Hew Health, a concierge medicine practice publishing from Destin and Orlando. Read across forty-seven states.