# The Cash-Pay Patient
*A field manual on what changes when insurance is not in the room — written by the person who designed the room that way.*
— Matthew Koucky · Hew Health · Vol I, Issue 05
---
When we designed Hew Health, the first thing I wanted to change about a traditional clinical visit was the silence we would replace with conversation. Not patient silence — administrative silence. No prior authorizations to chase. No coverage denials to appeal. No clinical decision shaped by what a payer would or would not pay for. No phone tree on the other end of a referral.
That silence, it turned out, was where the actual clinical work had been hiding.
## What insurance was doing to the visit
Before I founded the practice, I had been on both sides of the insured-medicine equation — as a patient, and watching my clinicians work inside it. Insurance shapes a clinical visit in ways most patients never notice because they happen so consistently. A few of them:
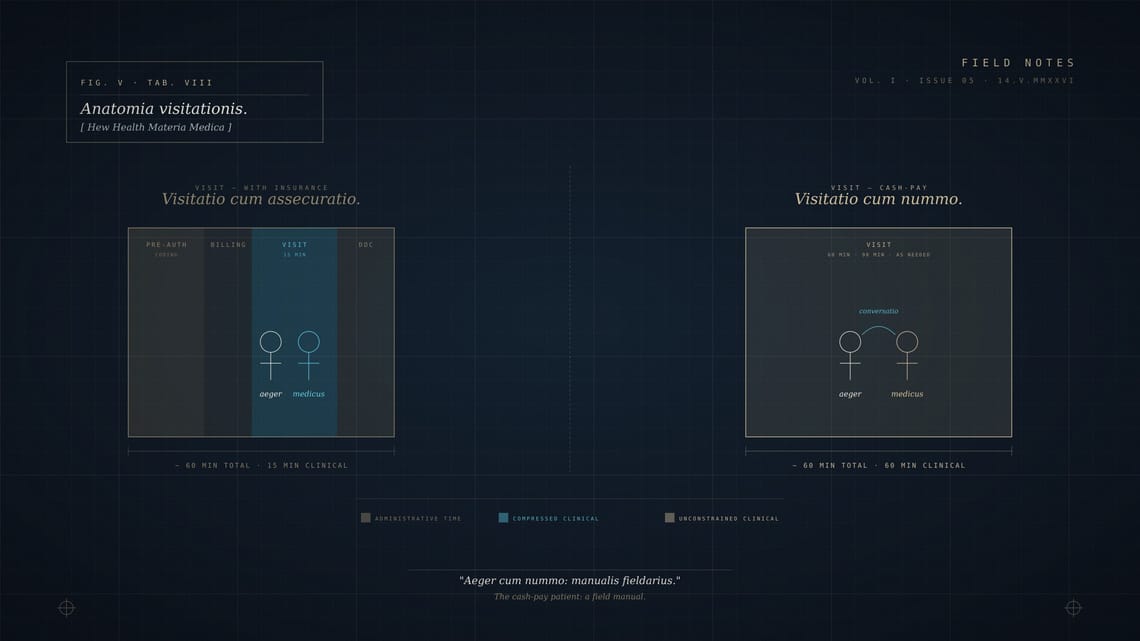
**The visit length is set by the billing code, not the problem.** A complex problem in a fifteen-minute slot gets compressed; a simple problem in a forty-minute slot gets stretched. Either way, the time was decided before the patient arrived.
**The medication formulary is set by the plan, not the practitioner.** Hours get spent on the phone with pharmacy benefits managers, arguing about why the medication the clinician prescribed is the medication the clinician prescribed.
**The lab panel is shaped by what is covered.** If a panel a clinician wants is not on the formulary, the patient either pays out of pocket for it or the clinician orders something close that the plan will cover. The second option is almost always inferior medicine and almost always what gets ordered.
**The follow-up cadence is shaped by reimbursement.** A patient who would benefit from being seen monthly gets seen quarterly because monthly visits are no longer reimbursable for their condition under their plan. Or the reverse: a patient who needs annual oversight gets in every three months because the practice needs the billable visits to stay solvent.
None of this is anyone's individual fault. It is the math of a system designed to ration care by making care expensive to deliver. The clinicians inside it are mostly doing the best work they can within the constraints. We built Hew Health to remove the constraints.
## What changes when you remove it
The first change is time. A visit that should be forty-five minutes is forty-five minutes. The patient who needs ninety gets ninety, and that ninety does not have to be split across three appointments to make the codes work. We schedule for the problem, not for the billing.
The second change is the medication conversation. The clinical team discusses what is right with the patient, and then they discuss what it costs. Sometimes the patient chooses a more expensive option because they can. Sometimes they choose a less expensive one because they have other priorities. The choice is theirs, made with real information, and the practice has no role in steering it toward what someone else will reimburse.
The third change is the lab conversation. Our clinicians order what they want to see, in the panel structure they want to see it in, on the cadence that matches the patient's protocol. If a patient wants to know what something will cost first, we tell them. Most are surprised by how reasonable our concierge bloodwork is once insurance is not in the markup chain.
The fourth change is the questions patients ask. Patients who have not been in cash-pay practices before will sometimes start the visit apologetically — sorry to bring this up, I know you're busy. They are used to being a billing event. Once they realize they are paying directly for our clinicians' time and that we have actually scheduled enough of it, the questions get longer, more specific, and more useful.
## What does not change
The clinical standards do not change. Cash-pay is not a license to do things that traditional medicine would not endorse. Most of the time our practice is delivering the same medicine that a careful in-network practitioner would practice, with the same evidence base and the same caution. The difference is the time to do it correctly.
The risk discussion does not change. If anything, it becomes more thorough — patients who are paying directly want to understand exactly what they are paying for and exactly what could go wrong. Our clinicians answer all of it.
The patient relationship does not change in *kind*, only in cadence. The same clinical instinct that built relationships with insured patients works here. The difference is that here our team can actually act on it.
## What we tell new patients
If you are coming to this from an insured practice and the cash-pay structure is new, the things worth knowing are these. The conversation will be longer than you are used to. You will be asked about parts of your life you may not have been asked about before — sleep, relationships, the work you actually do, how your weekends feel. The conversation is the medicine. The labs and protocols are how we measure whether the conversation is working.
You can also leave at any time. There is no contract that binds you to us beyond the one we honor by giving you what we said we would. If we are not the right practice for you, we will help you find one that is.
What we mostly want, on the first visit, is for you to talk and our clinicians to listen. That sentence is not marketing copy. It is the actual logic of the practice I built.
⁂
---
**Tags:** Cash-Pay · Practice Philosophy · Patient Experience · Field Manual · Founder Notes**Author:** Matthew Koucky**Category:** Field Manual**Read time:** ~7 min
---
*Field Notes is the editorial blog of Hew Health, a concierge medicine practice publishing from Destin and Orlando. Read across forty-seven states.*
The Cash-Pay Patient
# The Cash-Pay Patient *A field manual on what changes when insurance is not in the room — written by the person who designed the room that way.* — Matthew Koucky · Hew Health · Vol I, Issue 05 --- When we designed Hew Health, the first thing I wanted to change about a traditional
Field Notes · Vol. I
12.06.2026