# On Time Restoration
*The quiet logic of rotational optimization, and why we don't reach for the highest dose.*
— The Editorial · Hew Health · Vol I, Issue 03
---
A patient asked recently why, after six months of feeling progressively better, we were pulling back on his protocol. He was not unhappy. He was confused. The labs looked good, his sleep was excellent, his recovery from training had been the best of his adult life. Why would we change anything?
The honest answer is that we have watched too many patients optimize themselves into a corner. The protocol that produces the best six months is rarely the protocol that produces the best six years. The job is not to reach a peak. The job is to stay on the mountain.
## What the body does on its own
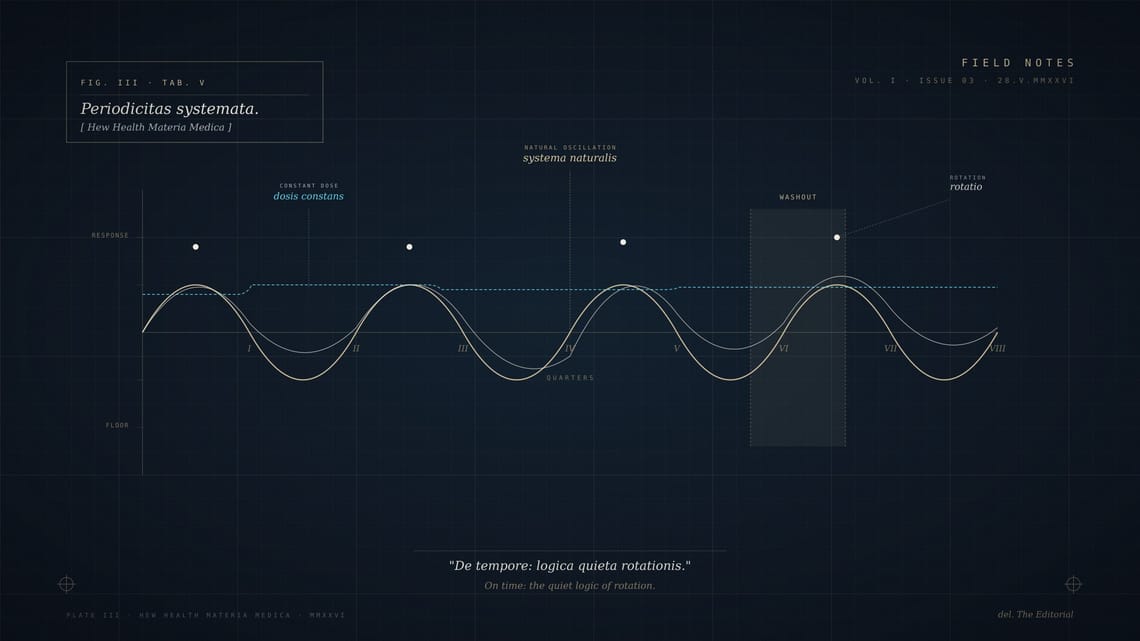
The endocrine system, left alone, does not run at a constant. It oscillates. Cortisol peaks in the morning and falls through the afternoon. Testosterone in men cycles weekly with a measurable variance, not just diurnally. Estrogen and progesterone in women run on a roughly twenty-eight-day arc that is too well-characterized to need restating. Even thyroid function has a small but real seasonal component.
The system is built to oscillate because oscillation is what keeps receptors sensitive. A signal that arrives constantly is a signal the body learns to ignore. A signal that varies — that rises, falls, returns — is one the body keeps listening for.
This is not controversial endocrinology. It is undergraduate physiology. What is sometimes lost is what it implies for how we prescribe.
## What constant supplementation does
If we layer a steady dose of any hormone over a system designed to oscillate, two things happen.
The first is mechanical: the steady dose flattens the natural rhythm. The morning peak that drives a patient out of bed gets smaller. The afternoon trough that lets the system reset gets smaller. The patient's range of feeling — the ordinary variation between *alert and slightly tired* — compresses. They start to feel uniformly OK rather than alive in the morning and ready to rest at night.
The second is receptor-level. Tissues exposed to constant signaling downregulate. The same dose, six months in, is producing less response than it did at month one. The standard answer is to raise the dose. The standard answer is wrong.
## What rotation looks like
In our practice we use the word *rotation* to describe a few different practices, all of which serve the same goal: keeping the patient's system responsive to what we are giving it.
The first is dosing rotation. We will run a protocol at a target dose for a quarter, then either reduce the dose by twenty to thirty percent for a month, or shift the timing of delivery, or both. The patient does not always notice. Their labs often shift in ways that confirm we did the right thing.
The second is class rotation. For some protocols — peptides especially — we will run agent A for three months, then agent B for two months, then return to A. This is not always possible. When it is, it almost always extends how long the protocol remains effective.
The third is intentional washout. Once a year, sometimes twice, we will take a patient off active supplementation for a defined window — typically two to four weeks — and observe. This is the most important rotation we do. It tells us what the patient's system is doing on its own, which is information we cannot get any other way.
## What we are titrating against
The replacement model titrates against the lab value. The optimization model titrates against the patient.
We describe what the patient should feel — present, sleeping, recovering, engaged with the people they live with — and we adjust the protocol until they describe themselves that way. Labs are the floor. They tell us we have not done anything chemically unwise. They are not the ceiling, and they are not, by themselves, the goal.
This means two patients with identical lab values may be on substantially different protocols. It also means a patient's protocol six months in is rarely the protocol they started on. We expect movement. We plan for it.
## The patient who asked
The patient mentioned at the start of this dispatch is, six weeks into the reduction, feeling slightly less perfect than he did at the peak — and considerably more like himself. The labs have shifted in the direction we expected. We will return him to the higher dose in another six weeks, and the response should be cleaner than it was the first time, because his system has not had the chance to get bored.
This is what we mean when we say time is part of the protocol. Not just the time the patient spends on a medication. The time we deliberately spend off it.
⁂
---
**Tags:** Hormone Optimization · Clinical Practice · Rotation · Method**Author:** The Editorial**Category:** Method**Read time:** ~7 min
---
*Field Notes is the editorial blog of Hew Health, a concierge medicine practice publishing from Destin and Orlando. Read across forty-seven states.*