# EBOO and the Limits of Inflammation Science
*An honest accounting of a therapy that has more story than literature, and what we keep and discard from each.*
— The Editorial · Hew Health · Vol I, Issue 08
---
Extracorporeal blood oxygenation and ozonation — EBOO — has a story problem. The patients who come asking about it know more about it than the published literature does. That is not their fault. The therapy has been used in Europe for decades, has a substantial body of clinical experience behind it, and has produced enough convincing outcomes in enough patients to keep a steady interest in the U.S. The published literature, particularly the kind a careful clinician would want to see — randomized, blinded, adequately powered — is sparse.
This dispatch is what we tell patients who ask about it. It is also what we tell other clinicians who ask why we offer it. The two conversations are similar enough to combine.
## What EBOO actually does
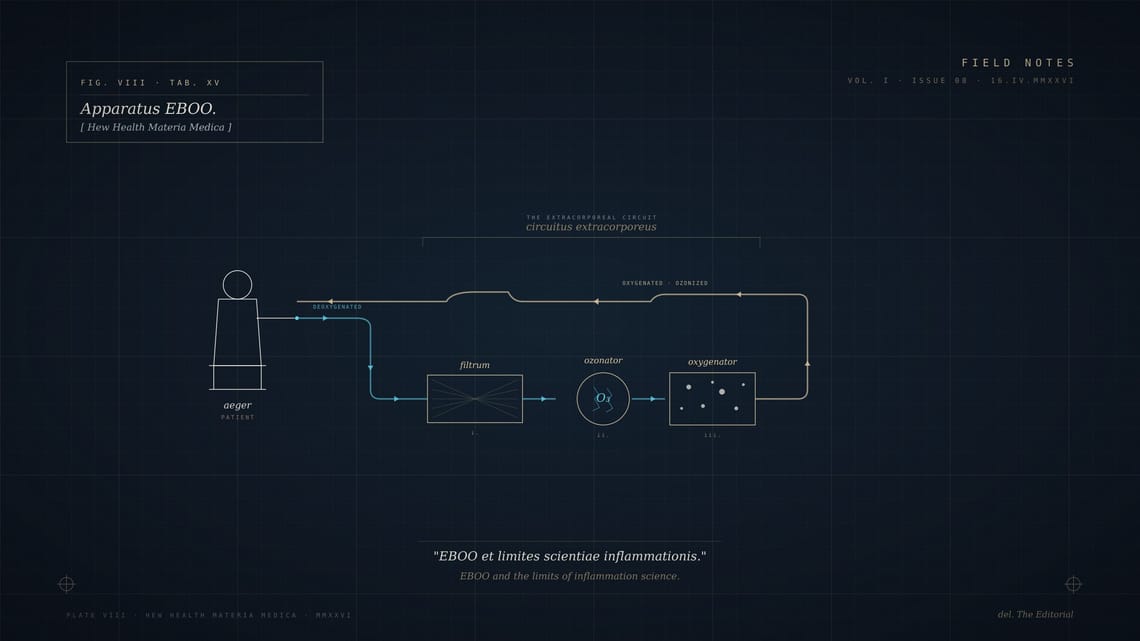
The procedure runs the patient's blood through an external circuit. The blood is briefly exposed to ozone and to higher concentrations of oxygen than it sees in normal circulation, then returned. The hypothesis — and it is a reasonable hypothesis with biochemistry behind it — is that the brief oxidative challenge produces a mild stress response in the patient's red cells and plasma proteins. That response, in turn, upregulates antioxidant systems, mitochondrial function, and certain immune signaling pathways for some window of time after the procedure.
The mechanism is not implausible. The body has well-characterized responses to oxidative stress, and brief, controlled stressors of various kinds (exercise, cold exposure, intermittent fasting) are widely accepted to produce beneficial adaptations through similar pathways. EBOO is, in a sense, a pharmacological version of the same logic.
## What the literature actually says
The honest version is: there is enough clinical data to suggest EBOO is safe when properly delivered, and enough mixed outcomes data to make any strong claim about specific conditions difficult to defend in print.
Some studies suggest measurable benefit in specific inflammatory conditions, peripheral vascular disease, certain autoimmune presentations, and chronic fatigue presentations. Some show modest benefit. Some show none. The methodology across studies varies enough that a meta-analysis is not particularly informative.
What we have not seen, and what would change the conversation considerably, is a large, well-controlled trial in a clearly defined patient population with clearly defined outcomes measured against a meaningful placebo. Until that exists, EBOO sits in the category of *plausible mechanism, mixed evidence, substantial clinical experience.*
## What we tell patients who ask
We will offer it. We will not oversell it. The conversation includes the following.
**The mechanism is real, but the magnitude of effect is uncertain.** Some patients describe substantial improvement in markers we can measure. Others describe modest improvement. A meaningful minority describe no perceptible change. We have not been able to predict which category any individual patient falls into ahead of time.
**It is not a treatment for a specific disease.** It is a systemic intervention with diffuse effects. If a patient comes in expecting that EBOO will treat their specific condition the way an antibiotic treats an infection, we redirect that expectation.
**It works best as part of a broader optimization program.** A patient on a thoughtful hormone protocol, sleeping well, training appropriately, eating in a way that does not produce constant inflammation, may see a clearer benefit from EBOO than a patient on no other intervention. We say this because we see it, not because the literature confirms it.
**The cost-benefit is the patient's to weigh.** EBOO is not inexpensive, particularly in a cash-pay practice. We give patients the cost openly, the range of likely outcomes openly, and let them decide.
## What we discard
There are claims about EBOO that do not survive contact with the actual evidence. We do not make them.
It is not a cure for cancer. It is not a guaranteed treatment for chronic Lyme. It is not a substitute for evidence-based medicine in conditions where evidence-based medicine works. Patients who arrive having read claims along those lines get a careful re-grounding before we go further.
We also discard the practice of running EBOO at high frequency over long periods. Most of our protocols are short series — typically three to six treatments over six to twelve weeks, then a pause, then a reassessment. The patient who is "doing EBOO weekly forever" has, in our view, mistaken the intervention for a maintenance therapy. It is not.
## The clinical question we are actually answering
When a patient asks about EBOO, the question underneath is usually something else. They are feeling worse than they think they should. Their conventional workup has not given them a clean answer. They have done their own reading and found EBOO. They are asking whether it might help.
The answer we give is rarely just *yes, here is the EBOO schedule*. The answer is usually some version of: let us look at the whole picture first, and EBOO may be one of several things we discuss. Sometimes EBOO is the right thing to do at the right time. Sometimes the right thing is to fix sleep, or test for something that has not been tested for, or simply to let a recent illness finish resolving.
The discipline of optimization medicine is knowing which question is the real one. EBOO is rarely the answer to the question the patient asks first. Sometimes it is the answer to the question they would have asked third.
## A closing note
What we will defend, without hesitation, is the practice's right to offer therapies that have substantial clinical experience and plausible mechanism even when the randomized trials are not yet what we would want them to be. The alternative — refusing to offer anything until the literature is complete — would have meant refusing to offer most of medicine through most of its history.
What we will not defend is offering them dishonestly. Patients deserve to know exactly what we know, exactly what we do not, and how we decided to offer something anyway. That is the conversation we try to have.
⁂
---
**Tags:** EBOO · Regenerative Medicine · Clinical Practice · Inflammation**Author:** The Editorial**Category:** Method**Read time:** ~8 min
---
*Field Notes is the editorial blog of Hew Health, a concierge medicine practice publishing from Destin and Orlando. Read across forty-seven states.*
EBOO and the Limits of Inflammation Science
# EBOO and the Limits of Inflammation Science *An honest accounting of a therapy that has more story than literature, and what we keep and discard from each.* — The Editorial · Hew Health · Vol I, Issue 08 --- Extracorporeal blood oxygenation and ozonation — EBOO — has a story problem. The patients who come
Field Notes · Vol. I
17.06.2026